
Viral Infections
Viral URTI is the most common predisposing factor for bacterial sinusitis. Rhinoviruses, influenza, and parainfluenza viruses are the most common causes of sinusitis.
The dynamic of sinusitis and other upper respiratory tract infections

Changes in the microbial etiology of sinusitis over time

Mechanism whereby viruses predispose to bacterial sinusitis
• Disruption of the local immune defense, leading to bacterial attachment to the epithelial cells.
• Production of several cytokines by infected epithelial cells. The activation of inflammatory pathways results in venous engorgement in the turbinates, leading to plasma leakage, discharge of goblet cells and seromucous glands, sneezing, and pain.
• Induction of cilia clearance malfunction, due to increased viscous material, slowing, and paralysis.
• Destructive epithelial damage.
• Infundibular and osteomeatal obstruction from mucosal swelling.
• Damage by influenza virus to epithelial cells, enhancing bacterial adherence.
• Direct synergy between the virus and potential pathogenic bacteria.
Human Rhinovirus

Interfering flora facts
• The “healthy” nasopharynx is generally colonized by nonpathogenic bacteria, some capable of interfering with the growth of potential pathogens through a mechanism called “bacterial interference.”
• Many interfering organisms produce bacteriocins (bactericidal proteins) and others compete on nutritional substrates.
• The nasopharynx of sinusitis-prone individuals is often colonized by potential pathogens, but rarely by interfering bacteria.
• Interfering organisms may play a role in the prevention of colonization by pathogens and the subsequent occurrence of sinusitis.
• Avoiding the use of antibiotics in viral infections and by using narrow spectrum antibiotics when possible can preserve the interfering organisms.
Role of normal interfering bacteria in preventing colonization by potential pathogens:

Balance between oropharyngeal pathogens and the interfering flora

Predominant organisms recovered in bacterial sinusitis | |||
Type of sinusitis | Aerobic bacteria | Anaerobic bacteria | Fungi |
Acute (community acquired) | Streptococcus pneumoniae | Peptostreptococcus spp. | |
Haemophilus influenzae* | |||
Moraxella catarrhalis* | |||
Acute (nosocomial) | Pseudomonas aeruginosa* | Peptostreptococcus spp. | |
Enterobacteria ceae* | Fusobacterium spp.* | ||
Staphylococcus aureus* | |||
Chronic | Staphylococcus aureus* | Pigmented Prevotella and Porphyromonas spp.* | Aspergillus spp. |
Streptococcus pneumoniae | Fusobacterium spp.* | Rhizopus spp. | |
Haemophilus influenzae* | Peptostreptococcus spp. | ||
*Organism capable of producing beta-lactamase. | |||
Gram stain of Streptococcus pneumoniae in pus:

Bacteria in Acute Bacterial Sinusitis
• Bacteria can be recovered from two thirds of patients.
• Bacteria recovered from pediatric and adult patients with community-acquired acute sinusitis are common respiratory pathogens: Streptococcus pneumoniae (25-30%), Haemophilus influenzae (30-40%), and Moraxella catarrhalis (15-30%).
• Staphylococcus aureus is the predominates in sphenoid sinusitis.
• Following the introduction of 7-valent S. pneumoniae vaccination in children the rate of the recovery of this organism decrease and that of H. influenzae increased.
• Beta-lactamase-producing strains of H. influenzae and M. catarrhalis were found in 20% and 27% of the cases, respectively.
•The rate of recovery of methicillin resistant Staphylococcus aureus (MRSA) has increased in the past decade in acute sinusitis (9% of all isolates). MRSA is more commonly recovered from smokers compared to non-smokers.
• The infection is polymicrobial in approximately one third of the cases. Enteric bacteria are found rarely.
• Anaerobic bacteria can be isolated in acute infections, generally in maxillary sinusitis associated with upper jaw molar infections.
• Anaerobes can be recovered from acute sinusitis associated with dental disease, generally as an extension of the infection from the roots of the upper premolar or molar teeth.
• Pseudomonas aeruginosa and other enteric gram-negative rods are common in nosocomial sinusitis (especially in patients who have nasal tubes, nasotracheal tubes, or catheters), the immunocompromised, and patients with HIV infection and cystic fibrosis.
Gram Stain of Haemophilus influenzae:

Bacterial etiology of acute maxillary bacterial sinusitis in children and adults | ||
Children (%) | Adults (%) | |
Streptococcus pneumoniae | 25–30 | 20–35 |
Haemophilus influenzae | 36–47 | 23–64 |
Moraxella catarrhalis | 27–32 | 19–60 |
Staphylococcus aureus | 0 | 0–1 |
Staphylococcus spp. | 6–9 | 6–17 |
Streptococcus spp. | 0 | 0–12 |
Anaerobic bacteria | 2 | 1–35 |
Enterobacteriaceae | 3 | 0–11 |
Bacteria in Chronic Bacterial Sinusitis
Anaerobic bacteria, Staphylococcus aureus, and aerobic gram-negative aerobes are the predominant pathogens. The rate of recovery of MRSA has increased in the past decade in chronic ( 14% of all isolates) sinusitis. MRSA is more commonly recovered from smokers compared to non-smokers.
Evidence supporting the role of anaerobes in chronic bacterial sinusitis
• Anaerobes were identified in chronic bacterial sinusitis whenever techniques for their cultivation were employed.
• The predominant isolates from patients with chronic bacterial sinusitis were pigmented Prevotella and Porphyromonas, Fusobacterium, and Peptostreptococcus spp. The predominant aerobic bacteria were S. aureus, M. catarrhalis, and H. influenzae.
• Elevated antibody levels (IgG) to two anaerobic organisms commonly recovered from sinus aspirates (Fusobacterium nucleatum and Prevotella intermedia) were detected in patients with chronic maxillary sinusitis, who harbor these organisms.71 Antibodies declined in those who responded to therapy, but did not decrease in those who failed therapy.

Serum antibodies to Prevotella and Fusobacterium in patients with chronic sinusitis before and after treatment
• Aerobic and anaerobic beta-lactamase-producing bacteria (BLPB) were isolated from more than one third of these patients. These were S. aureus, Haemophilus spp., Prevotella, and Fusobacterium spp.
A summary of 18 studies of chronic sinusitis, that included 1,758 patients (of which 133 were children) showed the recovery of anaerobes in 12% to 93% of the patients. The variability in recovery may result from differences in the methodologies used for transportation and cultivation, patient population, geography, and previous antimicrobial therapy.
Summary of 18 studies about the role of anaerobes in chronic bacterial sinusitis | |||||||||||||||||||||||||||||||
Reference | No. of patients | Condition | Patients from whom anaerobic organisms were isolated (%) | Organisms that were anaerobes* (%) | |||||||||||||||||||||||||||
1 | 83 | Chronic sinusitis | 75 | 52 | |||||||||||||||||||||||||||
2 | 66 | Acute and chronic sinusitis | 39 | 39 | |||||||||||||||||||||||||||
3 | 40 adults | Chronic sinusitis | 100 | 19 | |||||||||||||||||||||||||||
4 | 54 adults | Chronic sinusitis | 33 | 42 | |||||||||||||||||||||||||||
5 | 15 adults | Chronic sinusitis | 38 | 48 | |||||||||||||||||||||||||||
6 | 40 | Chronic sinusitis | 69 | 46 | |||||||||||||||||||||||||||
7 | 132 adults | Chronic sinusitis | NS | 22 | |||||||||||||||||||||||||||
8 | 35 | Chronic sinusitis | 70 | 39 | |||||||||||||||||||||||||||
9 | 40 children | Chronic sinusitis | 100 | 80 | |||||||||||||||||||||||||||
10 | 90 | Chronic sinusitis | 81 | 29 | |||||||||||||||||||||||||||
11 | 10 | Chronic maxillary sinusitis | 100 | 60 | |||||||||||||||||||||||||||
12 | 93 children | Chronic maxillary sinusitis | 93 | 93 | |||||||||||||||||||||||||||
13 | 126 adults | Chronic maxillary sinusitis | 90 | 88 | |||||||||||||||||||||||||||
14 | 68 adults | Chronic maxillary sinusitis | 100 | 82 | |||||||||||||||||||||||||||
15 | 190 adults | Chronic maxillary sinusitis | 150 | 68 | |||||||||||||||||||||||||||
16 | 114 adults | Acute and chronic sinusitis | NS | 12 | |||||||||||||||||||||||||||
17 | 412 | Chronic sinusitis | NS | 26 | |||||||||||||||||||||||||||
18 | 150 adults | Chronic maxillary sinusitis | 54 | 49 | |||||||||||||||||||||||||||
The microbiology of sinusitis according to the sinuses is listed below: Microbiology of acute and chronic sinusitis (percent of patients)
References: 1. Frederick J, Braude AI. Anaerobic infection of the paranasal sinuses. N Engl J Med 1974;290:135-7. 2. van Cauwenberge P, Verschraegen G, van Renterghem L. Bacteriological findings in sinusitis (1963-1975). Scand J Infect Dis Suppl 1976;9:72-7. 3. Karma P, Jokipii L, Sipila P, Luotonen J, Jokipii AMM. Bacteria in chronic maxillary sinusitis. Arch Otolaryngol 1979;105:386-90. 4. Berg O, Carenfelt C, Kronvall G. Bacteriology of maxillary sinusitis in relation to character of inflammation and prior treatment. Scand J Infect Dis 1988;20:511-6. 5. Fiscella RG, Chow JM. Cefixime for treatment of maxillary sinusitis. Am J Rhinol 1991;5:193-7. 6. Sedallian A, Bru JP, Gaillat J. Bacteriologic findings of chronic sinusitis [abstract no P2.71]. In: Program and Abstracts of the 17th International Congress on the Management of Infection ( 7. Simoncelli C, Ricci G, Molini E, von Garrel C, Capolunghi B, Giommetti S. Zur Bakterologie der chronischen Sinusitis Maxillaris. HNO 1992;40:16-8. 8. Tabaqchali S. Anaerobic infections of the head and neck region. Scand J Infect Dis 1988;57:24-34. 9. Brook I. Bacteriologic features of chronic sinusitis in children. JAMA 1981;246:967-9. 10. Hartog B, Degener JE, Van Benthem PP, Hordijk GJ. Microbiology of chronic maxillary sinusitis in adults: isolated aerobic and anaerobic bacteria and their susceptibility to 20 antibiotics. Acta Otolaryngol 1995;115:672-7. 11. Ito K, Ito Y, Mizuta K, et al. Bacteriology of chronic otitis media, chronic sinusitis, and paranasal mucopyocele in 12. Erkan M, Ozcan M, Arslan S, Soysal V, Bozdemir K, Haghighi N. Bacteriology of antrum in children with chronic maxillary sinusitis. Scand J Infect Dis 1996;28:283-5. 13. Erkan M, Aslan T, Ozcan M, Koc N. Bacteriology of antrum in adults with chronic sinusitis. Laryngoscope 1994;104(3 Pt 1):321-4. 14. Brook I, Thompson DH, Frazier EH. Microbiology and management of chronic maxillary sinusitis. Arch Otolaryngol Head Neck Surg 1994;120:1317-20. 15. Finegold SM, Wynne B, Rose FV, et al. Amoxicillin/clavulanate treatment of complicated sinusitis. Interscience Conference of Antimicrobial Agents and Chemotherapy, 2000 (Abstract #834). 16. Edelstein DR, Avner SE, Chow JM, et al. Once-a-day therapy for sinusitis: a comparison study of cefixime and amoxicillin. Laryngoscope 1993;103:33-41. 17. Klossek JM, Dubreuil L, Richet H, Richet B, Beutter P. Bacteriology of chronic purulent secretions in chronic rhinosinusitis. J Laryngol Otol 1998;112:1162-6. 18. Finegold SM, Flynn MJ, Rose FV, et al. Bacteriologic findings associated with chronic bacterial sinusitis in adults. Clin Infect Dis 2002;35:428-33. | |||||||||||||||||||||||||||||||
The transition from acute to chronic sinusitis was studied by repeated endoscopic aspirations of sinus secretions in patients who presented with acute maxillary sinusitis that did not respond to therapy.
• Most bacteria isolated from the first culture were aerobic or facultative bacteria (S. pneumoniae, H. influenzae, and M. catarrhalis).
• Failure to respond to therapy was associated with the emergence of resistant aerobic and anaerobic bacteria in subsequent aspirates (F. nucleatum, pigmented Prevotella and Porphyromonas spp., and Peptostreptococcus spp.)
• The infection was finally eradicated by antimicrobial agents effective against aerobic and anaerobic bacteria and, in some, also by surgical drainage.
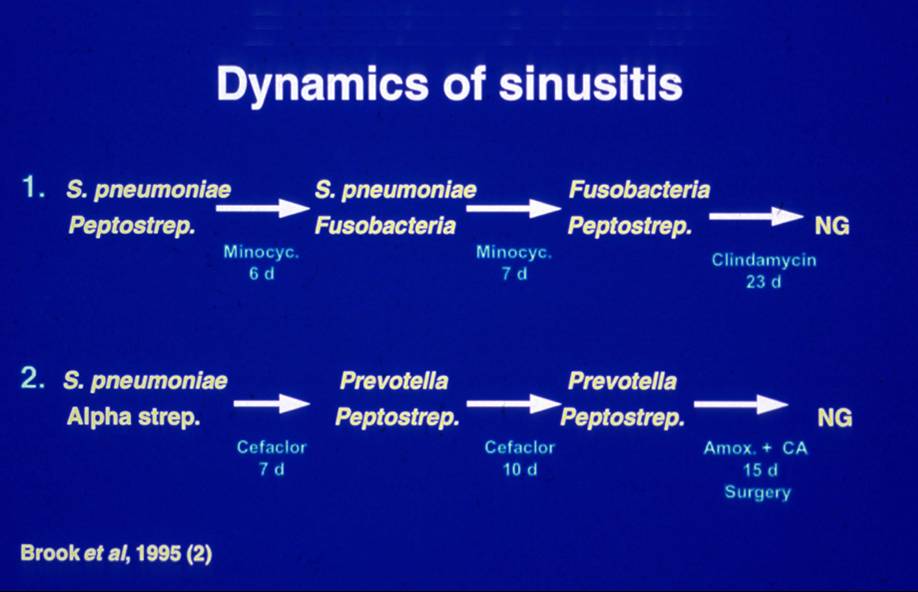
Dynamics of sinusitis showing the emergence of anaerobes as the infection progressed
Gram stain of Fusobacterium nucleatum:

Factors enhancing emergence of anaerobes in chronic bacterial sinusitis
• Selective pressure of antimicrobials enables resistant organisms to survive.
• The development of conditions appropriate for anaerobic growth:
a) Reduction in oxygen tension
b) Increase in acidity within the sinus
Persistent edema and swelling (reduces blood supply) and consumption of oxygen by anaerobic bacteria result in reduced oxygen tension and increased acidity within the sinus.
• The emergence over time or selection of anaerobes that possess virulence factors such as a capsule.

The origion of the anaerobic bacteria causing sinusitis is the oropharyngeal flora where they predominant outnumbering aerobic bacteria at a ration of 10-100 to 1.
More about the role of anaerobic bacteria can be found in the website devoted to these bacteria.

Oropharyngeal flora where anaerobes predominate
Characteristics of chronic bacterial sinusitis due to anaerobes
• Polymicrobial infection is common including sinusitis associated with nasal polyps.
• These infections are synergistic with mutual enhancement of bacterial growth.
• It can be more difficult to eradicate a mixed infection with narrow-spectrum antimicrobial agents, because of “protection” of penicillin-susceptible isolates by BLPB. This may contribute to chronicity.
AECS is defined as a sudden worsening of the baseline manifestation of chronic sinusitis with either worsening or appearance of new symptoms. Typically, the acute (not chronic) symptoms resolve completely between occurrences.
• The predominate aerobes are H. influenzae, S. pneumoniae, M. catarrhalis, S. aureus and K. pneumoniae.
• The predominate anaerobes are Prevotella and Porphyromonas, Peptostreptococcus, Fusobacterium spp., and Propionibacterium acnes.
• A change in the type of isolates was noted in all consecutive cultures obtained from the same individual, as different organisms emerged, and previously ones were no longer isolated.
• An increase in antimicrobial resistance can occur.
Nosocomial sinusitis
Nosocomial sinusitis often occurs in patients with extended periods of intensive care (postoperative patients, burn victims, patients with severe trauma) that involves prolonged endotracheal or nasogastric intubation.
• P. aeruginosa and other aerobic and facultative Gram-negative rods are common in nosocomial sinusitis (especially in patients who have nasal tubes or catheters), the immunocompromised, those with HIV, and those with cystic fibrosis.
• Patients with nasotracheal intubation for > 5 days are at a substantially risk for nosocomial sinusitis. In contrast to community-acquired sinusitis,
• The common pathogens are Gram-negative enteric bacteria (i.e., P. aeruginosa, K. pneumoniae, Enterobacter spp., Proteus mirabilis, Serratia marcescens) and Gram-positive cocci (occasionally streptococci and staphylococci).
• Anaerobes can also be recovered when methods for their isolation are performed.

Dental abscesses

Odontogenic sinusitis accounts for about 10% to 12% of cases of maxillary sinusitis.
• The microorganisms recovered from odontogenic infections generally reflect the indigenous oral microflora.
• Polymicrobial infection is common with 2-5 isolates per specimen, and 90% of the isolates were anaerobes in both acute and chronic infections.
• The predominant anaerobes were Prevotella, Porphyromonas, F. nucleatum, Peptostreptococcus and Fusobacterium spp.
• The predominant aerobes were a-hemolytic streptococci, and microaerophilic streptococci.
Dental infection from an upper molar can spread into the maxillary sinus


Chlamydia pneumoniae and Mycoplasma pneumoniae facts
• Role in bacterial sinusitis is uncertain.
• Serological evidence was found in only 2 of 103 patients with sinusitis and the organism was isolated in only one case from a sinus aspirate.
• An increase in antibody titers in one study suggests a possibility of co-infection and/or a possible etiologic link between bacterial sinusitis and Mycoplasma pneumoniae infection.
Fungal infection facts
• Fungi rarely cause community-acquired bacterial sinusitis.
• Fungi are common in patients with HIV, uncontrolled diabetes, and prolonged immunosuppressive therapy (especially transplant recipients) or following antimicrobial therapy.
• Aspergillus fumigatus is the most common fungal cause of sinusitis. It has been associated with smoking marijuana, as it contaminates the leaves. It can cause invasive, noninvasive, and disseminated sinusitis. Polymicrobial aerobic-anaerobic bacterial flora can be isolated in over 2/3 of fungal balls caused by Aspergillus spp.
Aspergillus fumigatus:

Fungal causes of bacterial sinusitis
• Aspergillus fumigatus, Aspergillus flavus, Aspergillus niger
• Schizophyllum commune
• Emericella nidulans
• Pseudallescheria boydii
• Paecilomyces spp.
• Candida spp.
• Mucor spp.
• Cryptococcus neoformans
• Penicillium melinii
• Scedosporium (Monosporium) apiospermum
• Blastomyces dermatitidis
• Bipolaris spp.
• Saprophytic fungi (Oreschslera spp. and Alternaria spp., Curvularia lunata, Exserohilum spp.)
Causes of allergic fungal bacterial sinusitis
• Alternaria spp.
• Aspergillus spp.
• Bipolaris spp.
• Chrysosporium spp.
• Drechslera spp.
• Exserohilum spp.
• Curvularia spp.
Organisms Recovered in Immunocompromised Patients
Patients with acquired or congenital immunodeficiency can be infected by organisms similar to those that infect nonimmunocompromised individuals as well as by unusual pathogens.
Organisms isolated in sinusitis in the immunocompromised host (in addition to organisms similar to those isolated in noncompromised patients) | |
Pseudomonas aeruginosa | Cytomegalovirus |
Staphylococcus aureus | Fungi: Candida, Aspergillus, Cryptococcus spp., Mucor |
Legionella spp. | Atypical mycobacteria |
Listeria monocytogenes | Microsporidium spp., Cryptosporidium spp., Acanthamoeba spp. |
Toxoplasma gondii | |